Heart Failure and Therapies
Pathology
According to the guidelines of the ESC, HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress. This is usually a myocardial abnormality causing systolic and/or diastolic ventricular dysfunction. However, abnormalities of the valves, pericardium, endocardium, heart rhythm and conduction can also cause HF (and more than one abnormality is often present). We use advanced computational models of cardiac function from the cell to organ levels to gain mechanistic insight into the processes of cardiac remodeling that trigger malignant ventricular arrhythmia, enhance abnormal diastolic/systolic biomechanics, and cause metabolic alterations in AVS patients.
Cardiac Resynchronization Therapy
Cardiac resynchronisation therapy is the insertion of electrodes in the left and right ventricles of the heart to treat heart failure by coordinating the function of the left and right ventricles via a pacemaker.
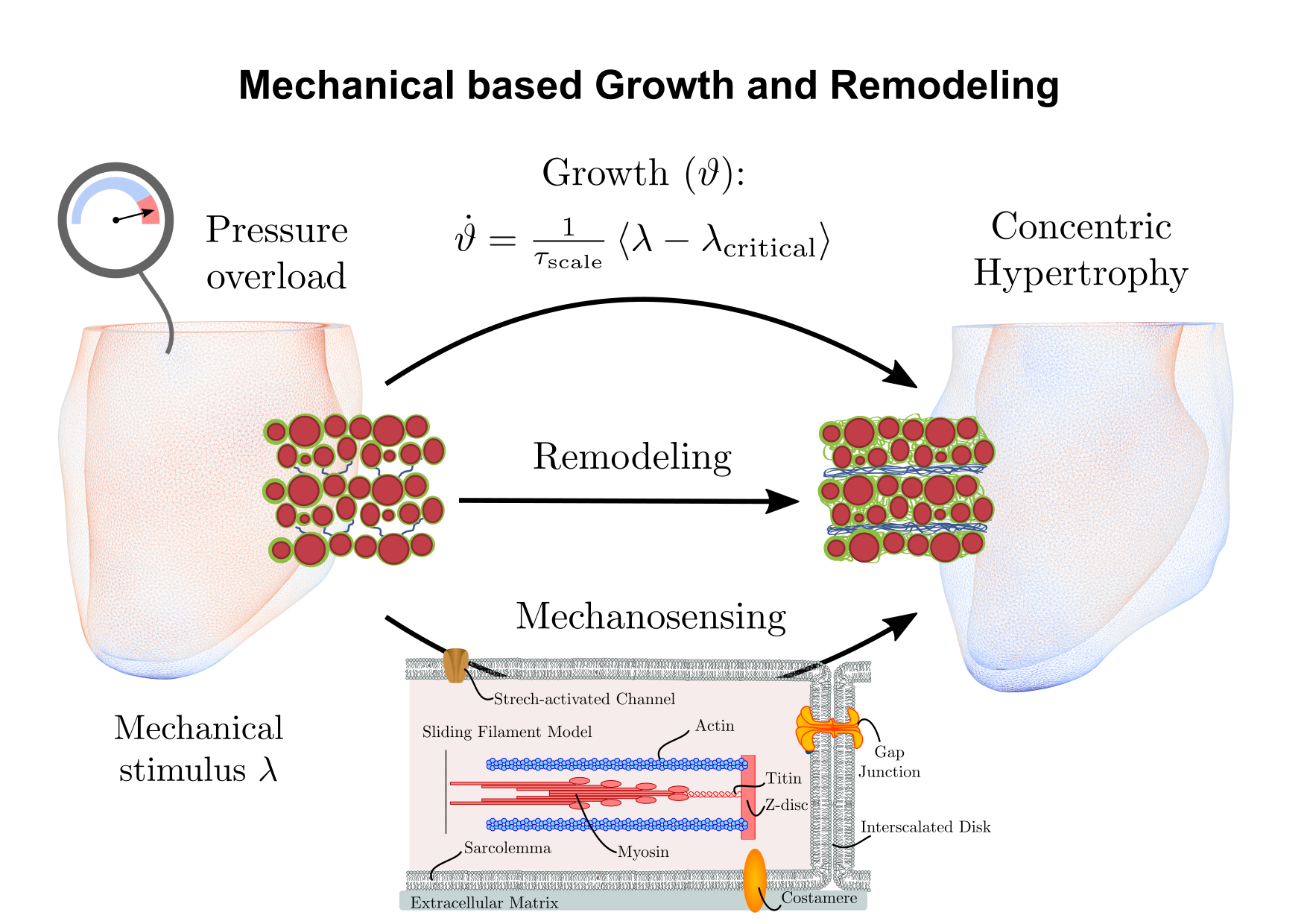
Growth and Remodeling
The myocardium can undergo both adaptive and maladaptive changes in response to altered states of the environment such as mechanical stimuli. This process is referred to as growth and remodeling (G&R). Many diseases of the heart include abnormal structural remodeling of the left ventricle (LV). Processes involve increased myocyte diameter and addition of myocytes, cell proliferation, apoptosis, and also increased collagen content, referred to as fibrosis. Initially, growth is a compensatory process to normalize the function on the heart to pathological stimuli such as aortic valve disease or hypertension. For example, in the case of pressure overload induced by aortic valve disease, these adaptive processes enhance systolic stiffness but also increase diastolic stiffness. Up to a certain time-point, these changes have been shown to be reversible. When pressure overload persists however, initially positive, adaptive changes may lead to cell necrosis and reparative fibrosis which bridges the gaps which originate from cell loss. Eventually, changes become irreversible and surgeries such as aortic valve replacement cannot prevent the progression towards heart failure. As G&R processes consist of countless pathways and their interaction, computational modeling has been recognized as a promising tool to investigate this problem.